
This site is intended for healthcare professionals.

In dermatology,
What You See Is Just The Beginning
because patient care goes beyond the surface.
Dermatologic care for patients goes beyond treating what's visible on the skin, and is often shaped by both underlying disease activity and the systems patients must navigate to receive care.
Chronic inflammatory skin conditions may remain active even between flares, requiring ongoing, individualized care.1 At the same time, outcomes are often shaped by factors beyond the exam room, including:
- Delays in recognition or referral2
- Limited access to specialists3
- Transportation challenges3
- Insurance complexity4
- Socioeconomic factors4
Sides of My Skin™ reflects a shared commitment to supporting a more comprehensive view of dermatologic care. Together, we can broaden the conversation to look beyond symptoms and recognize the many overlapping identities, needs and lived experiences that shape each person's skin and influence outcomes. For patients, it's not just about what's visible—it's the totality of their lived experiences.
Why This Matters
For many patients, particularly those managing multiple conditions or navigating healthcare systems with limited resources, systemic barriers may affect when care is initiated, how consistently it's maintained and whether follow-up occurs.
Recognizing these realities is an important step toward supporting more holistic, more inclusive and more personalized care.

Our Areas of Focus
Our earlier work highlighted gaps in care and system complexities that influence care experiences, particularly for diverse populations.
Now, our focus has expanded. Guided by insights from clinicians, patients and communities, we aim to address challenges affecting patients more broadly across settings and geographies, including:
Education & Awareness
Helping people better understand chronic skin conditions and what can affect care
Reducing Systemic Barriers
Addressing challenges like long wait times, limited specialist access and complex systems
Improving Timely Access to Care
Supporting earlier diagnosis, quicker referrals and consistent follow-up so patients can get care sooner
Community Engagement
Through community-based initiatives, including skin health education and sponsored outreach programs, we aim to complement clinical care by supporting awareness and connection outside traditional care settings.
We're working alongside healthcare professionals to support patients and help address gaps in education, navigation and access that may exist beyond the exam room.

Access downloadable resources to support community engagement.

HCP Educational Resources
Deepen your understanding of common dermatologic conditions.
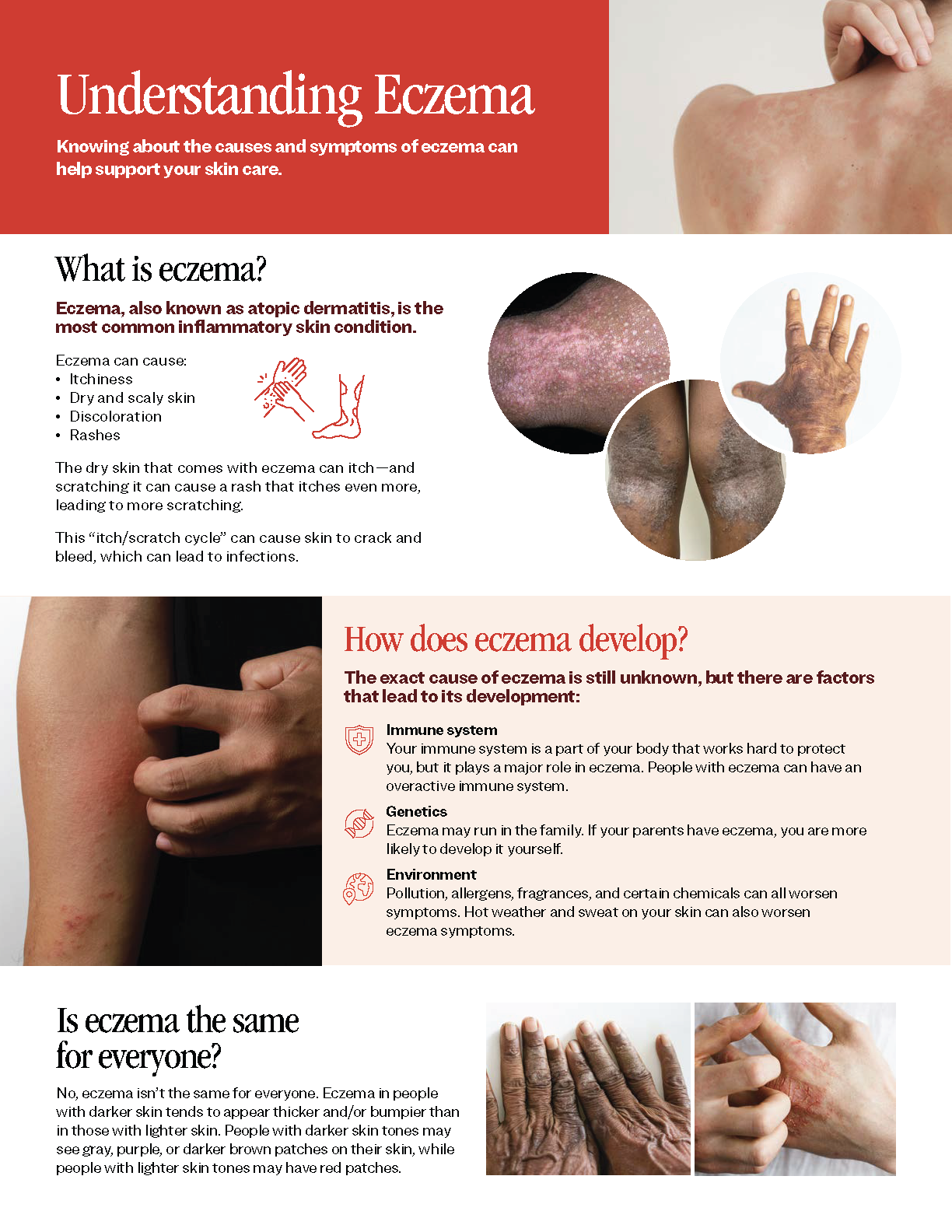
Atopic Dermatitis
From diagnosis to management of atopic dermatitis, discover important clinical insights and resources to support patients.
00:00-00:04
Music
00:05-00:09
Music
00:10-00:20
Music
00:21-00:30
Let's delve into Atopic Dermatitis, or AD, a chronic inflammatory condition of the skin marked by dysfunction of the epidermal barrier.1
00:31-00:51
Population-based studies within Europe and United States have found the highest prevalence of AD in Black ethnic groups at 19.3% compared with White and Hispanic ethnic groups at 16.1 and 7.8%, respectively.2
00:51-01:15
Studies predominantly based in the United States and United Kingdom suggest that patients with darker skin who have AD have a higher prevalence, a greater severity, a higher level and greater impact of pruritus, and higher prevalence of xerosis compared with those with lighter skin who have AD.2
01:16-01:28
Hispanic ethnicity and African American race are associated with increased odds of persistently active AD from childhood into adulthood.3
01:29-01:45
Let's explore the primary genetic factors influencing this condition. The diverse genetic background of different racial populations may contribute to the varying prevalence and persistence of AD.2,4
01:46-01:54
One of the most frequently studied genes in AD is FLG, a key component of the barrier function of the stratum corneum.1
01:55-02:11
FLG2 is another gene that encodes for the protein filaggrin-2, which also plays a key role in the skin barrier function; decreased expression of FLG2 is associated with lesional skin in AD and a thinner epidermis.1
02:12-02:22
Studies have shown that there are variations in the frequency of FLG and FLG2 mutation within and between racial or ethnic groups with AD.1
02:23-02:34
Loss-of-function or LoF mutations in either FLG or FLG2 lead to reduced filaggrin protein and result in impaired skin barrier function.1
02:35-03:10
The loss-of-function filaggrin mutation is shared among Asian and White individuals with AD, while loss-of-function FLG2 mutations are more common among Black individuals with AD.1
Furthermore, a greater downregulation of loricrin, a major protein in corneocytes, has been found in individuals of Black ethnicity2; this downregulation can contribute to the more severe and persistent nature of AD.
Studies have explored various molecular signatures unique to racial and ethnic groups with AD.1
03:11-03:32
Th1 activity is increased in the chronic stages of AD; the White population has the greatest Th1-related immune skewing; conversely, Th1 activation was largely absent in those with Black skin affected by AD, although it was present in affected individuals with Asian skin.2
03:33-03:58
Th17, Th22, and Th1 activation is also increased in the chronic stages of AD leading to epidermal thickening and abnormal keratinocyte differentiation demonstrated by more lichenified appearance; the literature suggests that those with Black skin who have AD have a robust increase in Th22 activity.2
03:59-04:12
Individuals of Black ethnicity with AD also have the highest IgE levels, correlating with disease severity, followed by those of Asian background, then White background.2
04:13-04:39
As we continue our exploration of AD and its impact across different ethnicities, it's essential to consider ethnic variations in skin.
Consensus statements on ethnic variations in normal skin barrier attribute differences between ethnicities to the variance in prevalence and severity of AD, xerosis, and pruritus.2
04:40-04:52
A higher prevalence of AD and ScORing Atopic Dermatitis severity score, (or SCORAD), after adjusting for erythema, has been reported in individuals of Black ethnicity compared with individuals of White ethnicity.2
04:53-05:23
Some studies show that Black skin has a higher transepidermal water loss that may contribute to impaired barrier function and increased severity of AD.1,2
Transepidermal water loss refers to the total amount of water vapor lost through the skin and has been a key estimate of stratum corneum barrier function.2
Transepidermal water loss, in combination with low ceramide levels, has been postulated to precipitate xerosis in people with darker skin types.2
05:24-05:46
Abnormalities in the amount and composition of ceramides has been associated with AD, specifically a reduced ceramide to cholesterol ratio.2
Lower ceramide levels and the ratio of ceramides to cholesterol in the stratum corneum may contribute to the increased disease severity experienced by some Black individuals with AD.1,2
05:47-06:14
Let's now examine how AD manifests clinically in patients with skin of color. AD may represent differently in Black, Asian, and Hispanic patients with a distinct papular or perifollicular morphology, violaceous or dark brown hyperpigmentation indicative of active disease, and more extensor or truncal involvement.3,5
06:14-06:40
Active disease in lighter skin can often present with patches and plaques that are pink to red and erythematous compared with brown to violaceous in darker skin.5
Morphology in darker skin can include follicular and papular presentations compared with patch and plaque morphology seen in lighter skin.5
Chronic disease in darker skin can also present with postinflammatory pigment change.5
06:41-07:09
Let's recap what we've learned about Atopic Dermatitis, or AD: AD is a chronic inflammatory skin condition caused primarily due to epidermal barrier dysfunction.1 It is more prevalent among Black, Hispanic, Asian and Pacific Islander populations, with Black ethnic groups showing the highest prevalence and severity, including increased pruritus and xerosis.1,2
07:10-08:07
We also discussed the role of genetic diversity in AD prevalence. Specifically, variations in the FLG and FLG2 genes are significant, with Black individuals often having FLG2 mutations, which, along with a higher Th22 activity, relates to greater disease severity. Ethnic differences also affect skin barrier function and ceramide levels, contributing to AD's severity.1,2
Ethnic differences in skin barrier function, including higher transepidermal water loss (TEWL) and altered ceramide levels, contribute to the increased severity of AD in darker skin types.1,2 These factors, combined with unique morphologies such as papular and perifollicular presentations in Black, Asian, and Hispanic patients, underscore the need for tailored therapeutic approaches.3,5
08:08-08:14
Understanding these variations is essential for effective management and treatment strategies across diverse populations.
Text on screen:
References:
1. Brown-Korsah JB, McKenzie S, Omar D, et al. Variations in genetics, biology, and phenotype of cutaneous disorders in skin of color - part I: genetic, biologic, and structural differences in skin of color. J Am Acad Dermatol. 2022;87(6):1239-1258
2. Gan C, Mahil S, Pink A, et al. Atopic dermatitis in skin of colour. Part 1: new discoveries in epidemiology and pathogenesis. Clin Exp Dermatol. 2023;48:609-616
3. McKenzie S, Brown-Korsah JB, Syder NC, et at. Variations in genetics, biology, and phenotype of cutaneous disorders in skin of color - part II: differences in clinical presentation and disparities in cutaneous disorders in skin of color. J Am Acad Dermatol. 2022;87(6):1261-1270.
4. Sachdeva M, Joseph M. Dermatology: how to manage atopic dermatitis in patients with skin of colour. Drugs Context. 2022;11:2021-12-1.
5. Taylor SC, Elbuluk NM. Taylor and Elbuluk’s Color Atlas and Synopsis for Skin of Color. McGraw Hill; 2023;2:11.
*Photo credit: SCIENCE PHOTO LIBRARY.
08:15-08:34
Music
08:35-08:47
Music
Key Dermatologic Conditions in Diverse Skin Tones: Atopic Dermatitis
Dr. McMichael explores the prevalence, insights, and the role of genetic diversity in atopic dermatitis (AD) as well as the need to tailor therapeutic approaches.
00:00-00:04
Music
00:05-00:09
Music
00:10-00:20
Music
00:21-00:30
Let's delve into Atopic Dermatitis, or AD, a chronic inflammatory condition of the skin marked by dysfunction of the epidermal barrier.1
00:31-00:51
Population-based studies within Europe and United States have found the highest prevalence of AD in Black ethnic groups at 19.3% compared with White and Hispanic ethnic groups at 16.1 and 7.8%, respectively.2
00:51-01:15
Studies predominantly based in the United States and United Kingdom suggest that patients with darker skin who have AD have a higher prevalence, a greater severity, a higher level and greater impact of pruritus, and higher prevalence of xerosis compared with those with lighter skin who have AD.2
01:16-01:28
Hispanic ethnicity and African American race are associated with increased odds of persistently active AD from childhood into adulthood.3
01:29-01:45
Let's explore the primary genetic factors influencing this condition. The diverse genetic background of different racial populations may contribute to the varying prevalence and persistence of AD.2,4
01:46-01:54
One of the most frequently studied genes in AD is FLG, a key component of the barrier function of the stratum corneum.1
01:55-02:11
FLG2 is another gene that encodes for the protein filaggrin-2, which also plays a key role in the skin barrier function; decreased expression of FLG2 is associated with lesional skin in AD and a thinner epidermis.1
02:12-02:22
Studies have shown that there are variations in the frequency of FLG and FLG2 mutation within and between racial or ethnic groups with AD.1
02:23-02:34
Loss-of-function or LoF mutations in either FLG or FLG2 lead to reduced filaggrin protein and result in impaired skin barrier function.1
02:35-03:10
The loss-of-function filaggrin mutation is shared among Asian and White individuals with AD, while loss-of-function FLG2 mutations are more common among Black individuals with AD.1
Furthermore, a greater downregulation of loricrin, a major protein in corneocytes, has been found in individuals of Black ethnicity2; this downregulation can contribute to the more severe and persistent nature of AD.
Studies have explored various molecular signatures unique to racial and ethnic groups with AD.1
03:11-03:32
Th1 activity is increased in the chronic stages of AD; the White population has the greatest Th1-related immune skewing; conversely, Th1 activation was largely absent in those with Black skin affected by AD, although it was present in affected individuals with Asian skin.2
03:33-03:58
Th17, Th22, and Th1 activation is also increased in the chronic stages of AD leading to epidermal thickening and abnormal keratinocyte differentiation demonstrated by more lichenified appearance; the literature suggests that those with Black skin who have AD have a robust increase in Th22 activity.2
03:59-04:12
Individuals of Black ethnicity with AD also have the highest IgE levels, correlating with disease severity, followed by those of Asian background, then White background.2
04:13-04:39
As we continue our exploration of AD and its impact across different ethnicities, it's essential to consider ethnic variations in skin.
Consensus statements on ethnic variations in normal skin barrier attribute differences between ethnicities to the variance in prevalence and severity of AD, xerosis, and pruritus.2
04:40-04:52
A higher prevalence of AD and ScORing Atopic Dermatitis severity score, (or SCORAD), after adjusting for erythema, has been reported in individuals of Black ethnicity compared with individuals of White ethnicity.2
04:53-05:23
Some studies show that Black skin has a higher transepidermal water loss that may contribute to impaired barrier function and increased severity of AD.1,2
Transepidermal water loss refers to the total amount of water vapor lost through the skin and has been a key estimate of stratum corneum barrier function.2
Transepidermal water loss, in combination with low ceramide levels, has been postulated to precipitate xerosis in people with darker skin types.2
05:24-05:46
Abnormalities in the amount and composition of ceramides has been associated with AD, specifically a reduced ceramide to cholesterol ratio.2
Lower ceramide levels and the ratio of ceramides to cholesterol in the stratum corneum may contribute to the increased disease severity experienced by some Black individuals with AD.1,2
05:47-06:14
Let's now examine how AD manifests clinically in patients with skin of color. AD may represent differently in Black, Asian, and Hispanic patients with a distinct papular or perifollicular morphology, violaceous or dark brown hyperpigmentation indicative of active disease, and more extensor or truncal involvement.3,5
06:14-06:40
Active disease in lighter skin can often present with patches and plaques that are pink to red and erythematous compared with brown to violaceous in darker skin.5
Morphology in darker skin can include follicular and papular presentations compared with patch and plaque morphology seen in lighter skin.5
Chronic disease in darker skin can also present with postinflammatory pigment change.5
06:41-07:09
Let's recap what we've learned about Atopic Dermatitis, or AD: AD is a chronic inflammatory skin condition caused primarily due to epidermal barrier dysfunction.1 It is more prevalent among Black, Hispanic, Asian and Pacific Islander populations, with Black ethnic groups showing the highest prevalence and severity, including increased pruritus and xerosis.1,2
07:10-08:07
We also discussed the role of genetic diversity in AD prevalence. Specifically, variations in the FLG and FLG2 genes are significant, with Black individuals often having FLG2 mutations, which, along with a higher Th22 activity, relates to greater disease severity. Ethnic differences also affect skin barrier function and ceramide levels, contributing to AD's severity.1,2
Ethnic differences in skin barrier function, including higher transepidermal water loss (TEWL) and altered ceramide levels, contribute to the increased severity of AD in darker skin types.1,2 These factors, combined with unique morphologies such as papular and perifollicular presentations in Black, Asian, and Hispanic patients, underscore the need for tailored therapeutic approaches.3,5
08:08-08:14
Understanding these variations is essential for effective management and treatment strategies across diverse populations.
Text on screen:
References:
1. Brown-Korsah JB, McKenzie S, Omar D, et al. Variations in genetics, biology, and phenotype of cutaneous disorders in skin of color - part I: genetic, biologic, and structural differences in skin of color. J Am Acad Dermatol. 2022;87(6):1239-1258
2. Gan C, Mahil S, Pink A, et al. Atopic dermatitis in skin of colour. Part 1: new discoveries in epidemiology and pathogenesis. Clin Exp Dermatol. 2023;48:609-616
3. McKenzie S, Brown-Korsah JB, Syder NC, et at. Variations in genetics, biology, and phenotype of cutaneous disorders in skin of color - part II: differences in clinical presentation and disparities in cutaneous disorders in skin of color. J Am Acad Dermatol. 2022;87(6):1261-1270.
4. Sachdeva M, Joseph M. Dermatology: how to manage atopic dermatitis in patients with skin of colour. Drugs Context. 2022;11:2021-12-1.
5. Taylor SC, Elbuluk NM. Taylor and Elbuluk’s Color Atlas and Synopsis for Skin of Color. McGraw Hill; 2023;2:11.
*Photo credit: SCIENCE PHOTO LIBRARY.
08:15-08:34
Music
08:35-08:47
Music

Duration 3:09
Beyond the Surface: Assessing Atopic Dermatitis in Patients with Diverse Skin Tones
Dr. Andrew Alexis discusses different ways to assess atopic dermatitis in patients with diverse skin tones.
Duration 2:08
Understanding Clinical Assessments of Atopic Dermatitis in Patients with Diverse Skin Tones
Dr. Andrew Alexis discusses clinical trials and scales used in assessing atopic dermatitis in patients with diverse skin tones.
Duration 1:58
Disease Severity and Care Delays in Patients with Diverse Skin Tones and Atopic Dermatitis
Dr. Andrew Alexis discusses disease severity and delays in care for patients with diverse skin tones and atopic dermatitis.
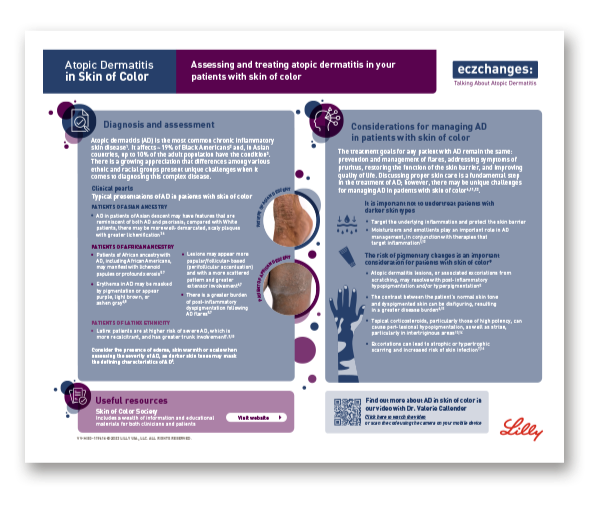
Eczchanges: Assessing and treating atopic dermatitis in your patients with diverse skin tones
A resource for health care professionals to effectively assess and treat atopic dermatitis (AD) in patients with diverse skin tones.
Psoriasis
Explore what psoriasis is, how it affects patients and how related comorbidities may impact care considerations.
00:04-00:09
Music
00:10-00:20
Music
00:11-00:28
In this chapter, we will explore the essential considerations for understanding psoriasis across different skin tones.
00:29-00:39
Psoriasis is a common, chronic, autoimmune, inflammatory skin disorder affecting patients from diverse ethnic groups with a wide spectrum of skin colors.1,2
00:40-01:14
Current epidemiologic estimates suggest that psoriasis is more prevalent in individuals with White skin compared with non-White skin.1,2
National Health and Nutrition Examination Surveys from 2003-2006 and 2009-2010 reported that the highest proportion of patients with psoriasis were White at 3.7%, followed by Black at 2.0% and Hispanic at 1.6%.2
01:15-01:47
However, psoriasis is likely to be underdiagnosed and underreported among African Americans and other individuals with skin of color due to variations in clinical presentation as well as disease distribution and severity.1,3 Statistics may also be underestimated due to underrepresentation of individuals with skin of color in clinical studies, with non-White participants comprising 14.2% of all adults enrolled in phase 3 trials in the United States.1
01:48-02:16
It is also important to note that the prevalence of psoriasis may vary by region, even between individuals with the same skin color. Such differences in prevalence may be attributed to genetic variations. For instance, African Americans are more closely related to West Africans, which may explain the comparably lower prevalence of psoriasis in individuals with Black skin in the data reported from the United States.2
02:17-02:33
Let's delve into the genetic factors contributing to psoriasis susceptibility across different ethnic groups.
A number of studies have shown differences in genetic susceptibility to psoriasis among ethnic groups.2
02:34-03:04
The HLA-Cw6 allele has been associated with guttate psoriasis, early-onset psoriasis, and psoriatic arthritis and an increased susceptibility for psoriasis in Asian and Middle Eastern populations.4
The HLA-Cw1 allele has been associated with pustular and erythrodermic psoriasis. It has also been associated with increased susceptibility to psoriasis and severity of psoriasis in Asian and Middle Eastern populations.4
03:05-03:28
Studies have shown that Asian individuals with psoriasis may be more likely to have higher levels of proinflammatory cytokines, such as IL-17A and IL-17 proinflammatory regulated cytokines (IL-8 and IL-1B), than White individuals with large plaque psoriasis.4
03:29-03:49
When examining the structural aspects of skin of color and the relation to psoriasis predisposition, no significant structural differences have been identified in skin of color that may impact predisposition across diverse patient populations.4
03:50-04:01
Let's explore the clinical presentation of psoriasis and how its features can vary across different skin tones.
04:02-04:27
Psoriasis typically presents with well-demarcated erythematous plaques with silvery scales.2
These plaques may vary in size, thickness, shape, degree of scaling, and distribution among different racial/ethnic groups.2,5
Black, Asian, and Hispanic patients with psoriasis tend to have thicker plaques with more scaling and body surface area involvement.1
04:28-05:04
In patients with skin of color, the active psoriatic lesions are more challenging to diagnose and could be mistaken for postinflammatory hyperpigmentation.2
In lighter skin, active disease is typically pink and red in contrast to being violaceous and brown in darker skin.5
Chronic treated psoriasis can result in dyspigmentation more commonly seen in skin of color, which can span the spectrum from postinflammatory hyperpigmentation to hypopigmentation and may take years to fade.1,2
05:05-05:33
To sum up our discussion on psoriasis, it's a chronic autoimmune skin disorder that affects people of all ethnicities, but it's more frequently reported in White individuals than in Black and Hispanic populations.1,2 However, psoriasis is often underdiagnosed in African Americans and other skin of color groups due to differences in symptom presentation and a lack of data.1,3
05:34-06:09
Genetic factors, like HLA-Cw6 and HLA-Cw1 alleles, play a role in psoriasis susceptibility, especially in Asian and Middle Eastern populations.4 Psoriasis typically presents as red plaques with silvery scales, but these can vary in size and thickness across ethnic groups.2,5 In skin of color, lesions may appear violaceous and brown, making diagnosis more challenging.5 Long-term treatment can also lead to pigmentation changes, which may persist for years.1,2
06:10-06:17
Understanding these differences is crucial for better diagnosing and treating psoriasis across diverse populations.
Text on screen:
References:
1. McKenzie S, Brown-Korsah JB, Syder NC, et at. Variations in genetics, biology, and phenotype of cutaneous disorders in skin of color - part II: differences in clinical presentation and disparities in cutaneous disorders in skin of color. J Am Acad Dermatol. 2022;87(6):1261-1270.
2. Lytvyn Y, Sachdeva M, Mufti A, et al. Dermatology: how to manage psoriasis and recognize differences in pathophysiology and presentation in patients with skin of colour. Drugs Context. 2022;11:2021-9-3.
3. Hermann AE, Nguyen DA, Wong CM, et al. Presentations of cutaneous disease in various skin pigmentations: plaque psoriasis. HCA Healthc J Med. 2022;3(3)139-144.
4. Brown-Korsah JB, McKenzie S, Omar D, et al. Variations in genetics, biology, and phenotype of cutaneous disorders in skin of color - part I: genetic, biologic, and structural differences in skin of color. J Am Acad Dermatol. 2022;87(6):1239-1258
5. Taylor SC, Elbuluk NM. Taylor and Elbuluk’s Color Atlas and Synopsis for Skin of Color. McGraw Hill; 2023;3:29.
*Photo credit: SCIENCE PHOTO LIBRARY.
06:18-06:24
Music
06:25-06:29
Music
Key Dermatologic Conditions in Diverse Skin Tones: Plaque Psoriasis
Dr. McMichael walks us through the differences in prevalence, clinical presentation across skin tones and diagnosis for psoriasis.
00:04-00:09
Music
00:10-00:20
Music
00:11-00:28
In this chapter, we will explore the essential considerations for understanding psoriasis across different skin tones.
00:29-00:39
Psoriasis is a common, chronic, autoimmune, inflammatory skin disorder affecting patients from diverse ethnic groups with a wide spectrum of skin colors.1,2
00:40-01:14
Current epidemiologic estimates suggest that psoriasis is more prevalent in individuals with White skin compared with non-White skin.1,2
National Health and Nutrition Examination Surveys from 2003-2006 and 2009-2010 reported that the highest proportion of patients with psoriasis were White at 3.7%, followed by Black at 2.0% and Hispanic at 1.6%.2
01:15-01:47
However, psoriasis is likely to be underdiagnosed and underreported among African Americans and other individuals with skin of color due to variations in clinical presentation as well as disease distribution and severity.1,3 Statistics may also be underestimated due to underrepresentation of individuals with skin of color in clinical studies, with non-White participants comprising 14.2% of all adults enrolled in phase 3 trials in the United States.1
01:48-02:16
It is also important to note that the prevalence of psoriasis may vary by region, even between individuals with the same skin color. Such differences in prevalence may be attributed to genetic variations. For instance, African Americans are more closely related to West Africans, which may explain the comparably lower prevalence of psoriasis in individuals with Black skin in the data reported from the United States.2
02:17-02:33
Let's delve into the genetic factors contributing to psoriasis susceptibility across different ethnic groups.
A number of studies have shown differences in genetic susceptibility to psoriasis among ethnic groups.2
02:34-03:04
The HLA-Cw6 allele has been associated with guttate psoriasis, early-onset psoriasis, and psoriatic arthritis and an increased susceptibility for psoriasis in Asian and Middle Eastern populations.4
The HLA-Cw1 allele has been associated with pustular and erythrodermic psoriasis. It has also been associated with increased susceptibility to psoriasis and severity of psoriasis in Asian and Middle Eastern populations.4
03:05-03:28
Studies have shown that Asian individuals with psoriasis may be more likely to have higher levels of proinflammatory cytokines, such as IL-17A and IL-17 proinflammatory regulated cytokines (IL-8 and IL-1B), than White individuals with large plaque psoriasis.4
03:29-03:49
When examining the structural aspects of skin of color and the relation to psoriasis predisposition, no significant structural differences have been identified in skin of color that may impact predisposition across diverse patient populations.4
03:50-04:01
Let's explore the clinical presentation of psoriasis and how its features can vary across different skin tones.
04:02-04:27
Psoriasis typically presents with well-demarcated erythematous plaques with silvery scales.2
These plaques may vary in size, thickness, shape, degree of scaling, and distribution among different racial/ethnic groups.2,5
Black, Asian, and Hispanic patients with psoriasis tend to have thicker plaques with more scaling and body surface area involvement.1
04:28-05:04
In patients with skin of color, the active psoriatic lesions are more challenging to diagnose and could be mistaken for postinflammatory hyperpigmentation.2
In lighter skin, active disease is typically pink and red in contrast to being violaceous and brown in darker skin.5
Chronic treated psoriasis can result in dyspigmentation more commonly seen in skin of color, which can span the spectrum from postinflammatory hyperpigmentation to hypopigmentation and may take years to fade.1,2
05:05-05:33
To sum up our discussion on psoriasis, it's a chronic autoimmune skin disorder that affects people of all ethnicities, but it's more frequently reported in White individuals than in Black and Hispanic populations.1,2 However, psoriasis is often underdiagnosed in African Americans and other skin of color groups due to differences in symptom presentation and a lack of data.1,3
05:34-06:09
Genetic factors, like HLA-Cw6 and HLA-Cw1 alleles, play a role in psoriasis susceptibility, especially in Asian and Middle Eastern populations.4 Psoriasis typically presents as red plaques with silvery scales, but these can vary in size and thickness across ethnic groups.2,5 In skin of color, lesions may appear violaceous and brown, making diagnosis more challenging.5 Long-term treatment can also lead to pigmentation changes, which may persist for years.1,2
06:10-06:17
Understanding these differences is crucial for better diagnosing and treating psoriasis across diverse populations.
Text on screen:
References:
1. McKenzie S, Brown-Korsah JB, Syder NC, et at. Variations in genetics, biology, and phenotype of cutaneous disorders in skin of color - part II: differences in clinical presentation and disparities in cutaneous disorders in skin of color. J Am Acad Dermatol. 2022;87(6):1261-1270.
2. Lytvyn Y, Sachdeva M, Mufti A, et al. Dermatology: how to manage psoriasis and recognize differences in pathophysiology and presentation in patients with skin of colour. Drugs Context. 2022;11:2021-9-3.
3. Hermann AE, Nguyen DA, Wong CM, et al. Presentations of cutaneous disease in various skin pigmentations: plaque psoriasis. HCA Healthc J Med. 2022;3(3)139-144.
4. Brown-Korsah JB, McKenzie S, Omar D, et al. Variations in genetics, biology, and phenotype of cutaneous disorders in skin of color - part I: genetic, biologic, and structural differences in skin of color. J Am Acad Dermatol. 2022;87(6):1239-1258
5. Taylor SC, Elbuluk NM. Taylor and Elbuluk’s Color Atlas and Synopsis for Skin of Color. McGraw Hill; 2023;3:29.
*Photo credit: SCIENCE PHOTO LIBRARY.
06:18-06:24
Music
06:25-06:29
Music
Duration 1:30
PsO Derm Week 2024 Video Snippet 3 - SoC
Explore comorbidities in psoriasis: focus on patients with skin of color with Dr. Jarell
PsO Comorbidity Infographic 1 - Skin of Color
Comorbidities in Psoriasis: Skin of Color
Alopecia Areata
Hear from experts about key diagnostic, management and clinical considerations for alopecia areata.
00:00-00:04
Music
00:05-00:09
Music
00:10-00:20
Music
00:20-00:30
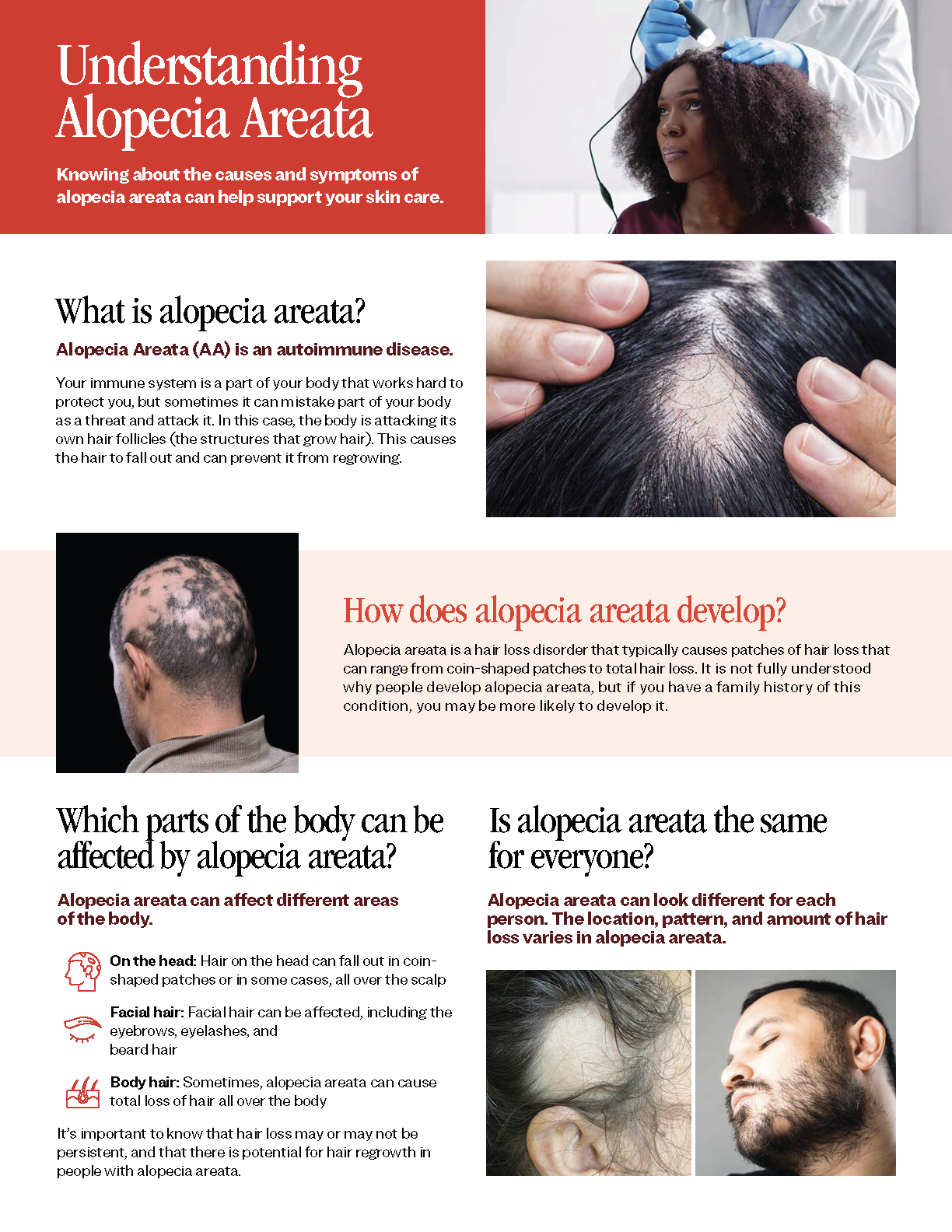
Let's explore Alopecia Areata or AA, an inflammatory disease of the follicular unit that results in nonscarring patches of hair loss.1
Text on screen: Amy McMichael, MD Atrium Health Wake Forest Baptist Dermatology
00:30-00:42
Circumscribed patches of hair loss occur most commonly on the scalp, eyebrows, eyelashes, and beard area, although any hair-bearing surface area may be involved.1
00:42-01:40
Several large epidemiologic studies have estimated that AA affects approximately 2% of the general population at some point during their lifetime.2
In a recent population-based study, the highest prevalence of AA was observed among Asian patients with 414 per 100,000 individuals, followed by Black patients at 226 per 100,000 individuals and Hispanic patients at 212 per 100,000.1
White patients had the lowest prevalence at 168 per 100,000 among the racial subgroups. Relative to White patients, prevalence ratios for Asian, Black, and Hispanic patients were 2.47, 1.35, and 1.26, respectively.1
01:40-01:56
Now, let's examine the genetic underpinnings of AA, focusing on how genetic variations may contribute to its prevalence, especially among individuals with darker skin tones.
01:56-02:10
AA is considered an autoimmune disease with a strong genetic component, and research suggests that certain genetic variations may be more prevalent in individuals with darker skin tones.3
02:10-02:34
In addition to well-known genes, such as PTPN22, CTLA4, and IL-2, which have been widely supported as being associated with AA, an increasing number of specific gene-related loci, for example, miRNAs, have been discovered through advances in genetic research.3
02:34-02:49
Mutations in STX17, the gene involved in melanin synthesis, has been associated with dark-colored hair, suggesting that STX17 may be associated with AA in patients with skin of color.3
02:49-03:05
Let's explore how the structural and biochemical properties of hair di[er among ethnic groups, and how these differences can influence susceptibility to conditions like alopecia.
03:05-03:34
Structural and biochemical characteristics of hair vary among ethnic groups.4
The chemical composition of the hair shaft, specifically the keratin and amino acid configurations, is similar across African, Asian, and Caucasian ethnicities; however, spiral hair is seen most in African hair, which makes the hair more difficult to comb and increases the risk of breakage due to styling.4
03:34-03:51
Fewer elastic fibers attaching hair follicles to the dermis in African hair compared with Caucasian hair has also been observed, which may help explain why certain types of alopecia occur more commonly in African than Caucasian individuals.4
03:51-04:04
Although the composition of various lipids in hair is similar across racial type, African hair appears to contain fewer lipids than Caucasian hair, increasing susceptibility to ultraviolet damage.4
04:04-04:25
In patients with AA, hair loss can take many forms ranging from hair loss in welldefined patches to diffuse or total hair loss, which can affect all hair-bearing sites. Patchy alopecia affecting the scalp is the most common type of AA.2
04:25-04:49
Alopecia is one of the most common dermatologic conditions affecting Black patients with a significant negative impact on quality of life. However, the lack of representation of patients with skin of color in the current literature may contribute to misdiagnosis, as some dermatologists may be unfamiliar with the clinical spectrum of alopecia presenting in darker scalps.5
04:49-05:34
Clinical presentation of AA in patients with skin of color may include hair thinning of varying severity on the scalp.5
Patches of nonscarring hair loss can be seen on any area of the scalp. Hair loss may also be seen in eyebrows, eyelashes, the beard area, and any area of the body. This is similar in all ethnicities.1
Trichoscopy may reveal perifollicular scale, erythema, and miniaturized hair.5
A honeycomb pigmentary network is seen commonly in Black patients and may be seen in AA as well.6
Histopathologic examination of biopsy specimens may demonstrate a lymphocytic infiltrate at the bulb on the hair follicle.6
05:34-05:49
Let's summarize our discussion on Alopecia Areata, or AA, an inflammatory autoimmune condition that causes nonscarring hair loss.1
05:49-06:35
It affects areas like the scalp, eyebrows, eyelashes, and beard, though it can occur on any hair-bearing surface.1 AA affects approximately 2% of the general population at some point during their lifetime, with the highest prevalence among Asian patients, followed by Black, Hispanic, and then White populations.1,2
Genetics play a key role, especially for those with darker skin tones. Genes like PTPN22, CTLA4, and IL-2, and new loci like miRNAs, are significant factors. The STX17 gene, related to melanin and dark hair, may also be linked to AA in skin of color.3
06:36-06:55
Hair's structural and biochemical differences across ethnic groups impact alopecia susceptibility. African hair, with fewer lipids and elastic fibers, may be more prone to certain alopecia types.4
Patchy alopecia affecting the scalp is the most common type of AA.2
06:55-07:01
I hope this has provided valuable insights into the complexities of AA across diverse populations.
Text on screen:
References:
1. Sy N, Mastacouris N, Strunk A, et al. Overall and racial and ethnic subgroup prevalences of alopecia areata, alopecia totalis, and alopecia universalis. JAMA Dermatol. 2023;159(4):419-423.
2. Pratt CH, King Jr LE, Messenger AG, et al. Alopecia areata. Nat Rev Dis Primers. 2017;3:17011.
3. Ho CY, Wu CY, Chen JYF, et al. Clinical and genetic aspects of alopecia areata: a cutting-edge review. Genes (Basel). 2023;14(7):1362.
4. Raffi J, Suresh R, Agbai O. Clinical recognition and management of alopecia in women of color. Int J Womens Dermatol. 2019;5:314-319.
5. Balazic E, Axler E, Nwankwo C, et al. Minimizing bias in alopecia diagnosis in skin of color patients. J Drugs Dermatol. 2023;22(7):703-705.
6. de Moura LH, Duque-Estrada B, Abraham LS, Barcaui CB, Sodre CT. Dermoscopy findings of alopecia areata in an African-American patient. J Dermatol Case Rep. 2008;2(4):52-54.
*Photo credit: SCIENCE PHOTO LIBRARY
07:01-07:08
Music
07:08-07:13
Music
Key Dermatologic Conditions in Diverse Skin Tones: Alopecia Areata
Dr. McMichael discusses alopecia areata (AA), its prevalence, the structural factors in AA predisposition, and the complexities of alopecia areata across diverse populations.
00:00-00:04
Music
00:05-00:09
Music
00:10-00:20
Music
00:20-00:30
Let's explore Alopecia Areata or AA, an inflammatory disease of the follicular unit that results in nonscarring patches of hair loss.1
Text on screen: Amy McMichael, MD Atrium Health Wake Forest Baptist Dermatology
00:30-00:42
Circumscribed patches of hair loss occur most commonly on the scalp, eyebrows, eyelashes, and beard area, although any hair-bearing surface area may be involved.1
00:42-01:40
Several large epidemiologic studies have estimated that AA affects approximately 2% of the general population at some point during their lifetime.2
In a recent population-based study, the highest prevalence of AA was observed among Asian patients with 414 per 100,000 individuals, followed by Black patients at 226 per 100,000 individuals and Hispanic patients at 212 per 100,000.1
White patients had the lowest prevalence at 168 per 100,000 among the racial subgroups. Relative to White patients, prevalence ratios for Asian, Black, and Hispanic patients were 2.47, 1.35, and 1.26, respectively.1
01:40-01:56
Now, let's examine the genetic underpinnings of AA, focusing on how genetic variations may contribute to its prevalence, especially among individuals with darker skin tones.
01:56-02:10
AA is considered an autoimmune disease with a strong genetic component, and research suggests that certain genetic variations may be more prevalent in individuals with darker skin tones.3
02:10-02:34
In addition to well-known genes, such as PTPN22, CTLA4, and IL-2, which have been widely supported as being associated with AA, an increasing number of specific gene-related loci, for example, miRNAs, have been discovered through advances in genetic research.3
02:34-02:49
Mutations in STX17, the gene involved in melanin synthesis, has been associated with dark-colored hair, suggesting that STX17 may be associated with AA in patients with skin of color.3
02:49-03:05
Let's explore how the structural and biochemical properties of hair di[er among ethnic groups, and how these differences can influence susceptibility to conditions like alopecia.
03:05-03:34
Structural and biochemical characteristics of hair vary among ethnic groups.4
The chemical composition of the hair shaft, specifically the keratin and amino acid configurations, is similar across African, Asian, and Caucasian ethnicities; however, spiral hair is seen most in African hair, which makes the hair more difficult to comb and increases the risk of breakage due to styling.4
03:34-03:51
Fewer elastic fibers attaching hair follicles to the dermis in African hair compared with Caucasian hair has also been observed, which may help explain why certain types of alopecia occur more commonly in African than Caucasian individuals.4
03:51-04:04
Although the composition of various lipids in hair is similar across racial type, African hair appears to contain fewer lipids than Caucasian hair, increasing susceptibility to ultraviolet damage.4
04:04-04:25
In patients with AA, hair loss can take many forms ranging from hair loss in welldefined patches to diffuse or total hair loss, which can affect all hair-bearing sites. Patchy alopecia affecting the scalp is the most common type of AA.2
04:25-04:49
Alopecia is one of the most common dermatologic conditions affecting Black patients with a significant negative impact on quality of life. However, the lack of representation of patients with skin of color in the current literature may contribute to misdiagnosis, as some dermatologists may be unfamiliar with the clinical spectrum of alopecia presenting in darker scalps.5
04:49-05:34
Clinical presentation of AA in patients with skin of color may include hair thinning of varying severity on the scalp.5
Patches of nonscarring hair loss can be seen on any area of the scalp. Hair loss may also be seen in eyebrows, eyelashes, the beard area, and any area of the body. This is similar in all ethnicities.1
Trichoscopy may reveal perifollicular scale, erythema, and miniaturized hair.5
A honeycomb pigmentary network is seen commonly in Black patients and may be seen in AA as well.6
Histopathologic examination of biopsy specimens may demonstrate a lymphocytic infiltrate at the bulb on the hair follicle.6
05:34-05:49
Let's summarize our discussion on Alopecia Areata, or AA, an inflammatory autoimmune condition that causes nonscarring hair loss.1
05:49-06:35
It affects areas like the scalp, eyebrows, eyelashes, and beard, though it can occur on any hair-bearing surface.1 AA affects approximately 2% of the general population at some point during their lifetime, with the highest prevalence among Asian patients, followed by Black, Hispanic, and then White populations.1,2
Genetics play a key role, especially for those with darker skin tones. Genes like PTPN22, CTLA4, and IL-2, and new loci like miRNAs, are significant factors. The STX17 gene, related to melanin and dark hair, may also be linked to AA in skin of color.3
06:36-06:55
Hair's structural and biochemical differences across ethnic groups impact alopecia susceptibility. African hair, with fewer lipids and elastic fibers, may be more prone to certain alopecia types.4
Patchy alopecia affecting the scalp is the most common type of AA.2
06:55-07:01
I hope this has provided valuable insights into the complexities of AA across diverse populations.
Text on screen:
References:
1. Sy N, Mastacouris N, Strunk A, et al. Overall and racial and ethnic subgroup prevalences of alopecia areata, alopecia totalis, and alopecia universalis. JAMA Dermatol. 2023;159(4):419-423.
2. Pratt CH, King Jr LE, Messenger AG, et al. Alopecia areata. Nat Rev Dis Primers. 2017;3:17011.
3. Ho CY, Wu CY, Chen JYF, et al. Clinical and genetic aspects of alopecia areata: a cutting-edge review. Genes (Basel). 2023;14(7):1362.
4. Raffi J, Suresh R, Agbai O. Clinical recognition and management of alopecia in women of color. Int J Womens Dermatol. 2019;5:314-319.
5. Balazic E, Axler E, Nwankwo C, et al. Minimizing bias in alopecia diagnosis in skin of color patients. J Drugs Dermatol. 2023;22(7):703-705.
6. de Moura LH, Duque-Estrada B, Abraham LS, Barcaui CB, Sodre CT. Dermoscopy findings of alopecia areata in an African-American patient. J Dermatol Case Rep. 2008;2(4):52-54.
*Photo credit: SCIENCE PHOTO LIBRARY
07:01-07:08
Music
07:08-07:13
Music
Duration 4:31
Alopecia Areata in Black Patients: Clinical Pearls presented by Dr. Victoria Barbosa
Dr. Victoria Barbosa provides clinical insights to educate dermatologists about special considerations in the diagnosis and management of alopecia areata in black patients.

Duration 1:26
Alopecia Areata in Black Patients: Module 1 - Traction Alopecia and Alopecia Areata
Dr. Victoria Barbosa shares clinical insights regarding traction alopecia and alopecia areata in black patients.
Duration 1:18
Alopecia Areata in Black Patients: Module 2 - Alopecia Can Be Multifactorial
Dr. Victoria Barbosa discusses how alopecia can be multifactorial and shares clinical pearls for dermatologists.
Duration 1:50
Alopecia Areata in Black Patients: Module 3 - Diagnostic Pitfalls in Alopecia Areata
Dr. Victoria Barbosa provides clinical considerations regarding two diagnostic pitfalls for alopecia areata in black women.
Hidradenitis Suppurativa
Deepen your understanding of what causes hidradenitis suppurativa (HS) and explore how genetic factors contribute to the severity and appearance of it.
00:00-00:03
Music
00:04-00:09
Music
00:05-00:20
Music
00:21-00:40
Let's delve into the complex nature of Hidradenitis Suppurativa, or HS, a chronic, debilitating condition characterized by recurrent, inflammatory subcutaneous nodules, draining sinus tracts, and chronic scarring primarily affecting the axilla, groin, and inframammary regions.1,2
00:41-01:11
Estimates of HS prevalence vary from 0.05% to 4% in the general population, but it is known that race significantly affects the prevalence of the disease.3
Black patients have the highest rate of prevalence of HS, and studies have reported an increased prevalence in African and Hispanic populations, as well as in women.1,4
01:12-01:46
African Americans with HS may have a different disease profile. For example, a US study reveled differences in Charleston Comorbidity Index scores with 2.89 in African Americans vs 1.79 in Whites, indicating a higher predicted risk of death. Additionally, a single institution study in New York reported a significantly higher Hurley stage of disease in African Americans, indicating more severe disease.3
01:47-02:13
Let's examine the genetic and molecular underpinnings of HS across various ethnic groups.
We'll focus on the role of y-secretase mutations in the disease's pathogenesis and explore how these genetic factors influence treatment responses, particularly in populations of Asian, Black, and Middle Eastern descent.
02:14-02:32
Familial and sporadic forms of HS in Asian individuals including Chinese, Singaporean Chinese, Japanese, and East Indian as well as in Black, and Middle Eastern individuals have implicated mutations in γ-secretase in the pathogenesis of HS.2
02:33-02:55
Mutations in y-secretase result in epithelial keratinocyte hyperplasia and follicular hyperkeratosis, which are associated with HS.
Preliminary studies have shown that the incidence of γ-secretase mutations may be higher among some Asian populations with HS than among White populations.2
02:56-03:17
Now, let's focus on the anatomical and physiological factors contributing to HS, particularly in areas rich in apocrine glands.2
HS lesions predominantly affect the apocrine gland-bearing areas of the body.2
03:18-03:37
The pathogenesis of HS is thought to involve follicular hyperkeratosis with subsequent occlusion and dilatation of the hair follicle, leading to rupture, inflammation, abscess formation, and, despite possible disease remission, dermal contractures and disfiguring scars.2,4
03:38-03:58
In several studies, Black individuals were reported to have larger, more numerous, and more productive apocrine glands than White individuals.2
An anatomic predisposition for larger apocrine glands may explain, in part, the increased prevalence and severity of HS in Black patients.2
03:59-04:42
Let's explore the clinical presentation of HS across different racial groups.
There are currently no major differences in morphologic presentation across the races in the literature.1
However, keloidal scarring is a complication more frequently seen among Black, Asian, and Hispanic patients in later stages of the disease.1,5
HS typically affects intertriginous skin, and buttock involvement is associated with increased disease severity.1
In lighter skin, lesions can be seen as pink to red in color in contrast to the violaceous or brawny appearance in skin of color.5
04:43-05:53
Let's summarize our key points on Hidradenitis Suppurativa or HS.
This chronic skin condition causes painful nodules and scarring, primarily in areas like the armpits and groin.1,2 It affects more Black, African, Hispanic populations and women, with African Americans often experiencing more severe cases.1,3,4
Genetic mutations in y-secretase are linked to HS, particularly in Asian, Black, and Middle Eastern groups.2 These mutations lead to epithelial keratinocyte hyperplasia and follicular hyperkeratosis.2
HS affects areas with many apocrine glands, which are larger in Black individuals, possibly explaining higher disease prevalence and severity.2
While lesion appearance is generally similar across races, keloidal scarring is more common in Black, Asian, and Hispanic patients.1,5
Lesions appear pink to red in lighter skin and more purplish or brown in darker skin.5
05:54-06:02
Recognizing these variations is key to better diagnose and care for HS patients across diverse backgrounds.
Text on screen:
References:
1. McKenzie S, Brown-Korsah JB, Syder NC, et at. Variations in genetics, biology, and phenotype of cutaneous disorders in skin of color - part II: differences in clinical presentation and disparities in cutaneous disorders in skin of color. J Am Acad Dermatol. 2022;87(6):1261-1270.
2. Brown-Korsah JB, McKenzie S, Omar D, et al. Variations in genetics, biology, and phenotype of cutaneous disorders in skin of color - part I: genetic, biologic, and structural differences in skin of color. J Am Acad Dermatol. 2022;87(6):1239-1258
3. Kilgour JM, Li S, Sarin KY. Hidradenitis suppurativa in patients of color is associated with increased disease severity and healthcare utilization: a retrospective analysis of 2 US cohorts. JAAD Int. 2021;3:42-52.
4. Lee DE, Clark AK, Shi VY. Hidradenitis suppurativa: disease burden and atiology in skin of color. Dermatology. 2018;233(6):456-461.
5. Taylor SC, Elbuluk NM. Taylor and Elbuluk’s Color Atlas and Synopsis for Skin of Color. McGraw Hill; 2023;23:167.
*Photo credit: SCIENCE PHOTO LIBRARY.
06:03-06:09
Music
06:09-06:13
Music
Key Dermatologic Conditions in Diverse Skin Tones: Hidradenitis Suppurativa
Dr. McMichael delves into the complex nature of Hidradenitis Suppurativa (HS) including the differences in disease profiles and clinical presentation across diverse backgrounds.
00:00-00:03
Music
00:04-00:09
Music
00:05-00:20
Music
00:21-00:40
Let's delve into the complex nature of Hidradenitis Suppurativa, or HS, a chronic, debilitating condition characterized by recurrent, inflammatory subcutaneous nodules, draining sinus tracts, and chronic scarring primarily affecting the axilla, groin, and inframammary regions.1,2
00:41-01:11
Estimates of HS prevalence vary from 0.05% to 4% in the general population, but it is known that race significantly affects the prevalence of the disease.3
Black patients have the highest rate of prevalence of HS, and studies have reported an increased prevalence in African and Hispanic populations, as well as in women.1,4
01:12-01:46
African Americans with HS may have a different disease profile. For example, a US study reveled differences in Charleston Comorbidity Index scores with 2.89 in African Americans vs 1.79 in Whites, indicating a higher predicted risk of death. Additionally, a single institution study in New York reported a significantly higher Hurley stage of disease in African Americans, indicating more severe disease.3
01:47-02:13
Let's examine the genetic and molecular underpinnings of HS across various ethnic groups.
We'll focus on the role of y-secretase mutations in the disease's pathogenesis and explore how these genetic factors influence treatment responses, particularly in populations of Asian, Black, and Middle Eastern descent.
02:14-02:32
Familial and sporadic forms of HS in Asian individuals including Chinese, Singaporean Chinese, Japanese, and East Indian as well as in Black, and Middle Eastern individuals have implicated mutations in γ-secretase in the pathogenesis of HS.2
02:33-02:55
Mutations in y-secretase result in epithelial keratinocyte hyperplasia and follicular hyperkeratosis, which are associated with HS.
Preliminary studies have shown that the incidence of γ-secretase mutations may be higher among some Asian populations with HS than among White populations.2
02:56-03:17
Now, let's focus on the anatomical and physiological factors contributing to HS, particularly in areas rich in apocrine glands.2
HS lesions predominantly affect the apocrine gland-bearing areas of the body.2
03:18-03:37
The pathogenesis of HS is thought to involve follicular hyperkeratosis with subsequent occlusion and dilatation of the hair follicle, leading to rupture, inflammation, abscess formation, and, despite possible disease remission, dermal contractures and disfiguring scars.2,4
03:38-03:58
In several studies, Black individuals were reported to have larger, more numerous, and more productive apocrine glands than White individuals.2
An anatomic predisposition for larger apocrine glands may explain, in part, the increased prevalence and severity of HS in Black patients.2
03:59-04:42
Let's explore the clinical presentation of HS across different racial groups.
There are currently no major differences in morphologic presentation across the races in the literature.1
However, keloidal scarring is a complication more frequently seen among Black, Asian, and Hispanic patients in later stages of the disease.1,5
HS typically affects intertriginous skin, and buttock involvement is associated with increased disease severity.1
In lighter skin, lesions can be seen as pink to red in color in contrast to the violaceous or brawny appearance in skin of color.5
04:43-05:53
Let's summarize our key points on Hidradenitis Suppurativa or HS.
This chronic skin condition causes painful nodules and scarring, primarily in areas like the armpits and groin.1,2 It affects more Black, African, Hispanic populations and women, with African Americans often experiencing more severe cases.1,3,4
Genetic mutations in y-secretase are linked to HS, particularly in Asian, Black, and Middle Eastern groups.2 These mutations lead to epithelial keratinocyte hyperplasia and follicular hyperkeratosis.2
HS affects areas with many apocrine glands, which are larger in Black individuals, possibly explaining higher disease prevalence and severity.2
While lesion appearance is generally similar across races, keloidal scarring is more common in Black, Asian, and Hispanic patients.1,5
Lesions appear pink to red in lighter skin and more purplish or brown in darker skin.5
05:54-06:02
Recognizing these variations is key to better diagnose and care for HS patients across diverse backgrounds.
Text on screen:
References:
1. McKenzie S, Brown-Korsah JB, Syder NC, et at. Variations in genetics, biology, and phenotype of cutaneous disorders in skin of color - part II: differences in clinical presentation and disparities in cutaneous disorders in skin of color. J Am Acad Dermatol. 2022;87(6):1261-1270.
2. Brown-Korsah JB, McKenzie S, Omar D, et al. Variations in genetics, biology, and phenotype of cutaneous disorders in skin of color - part I: genetic, biologic, and structural differences in skin of color. J Am Acad Dermatol. 2022;87(6):1239-1258
3. Kilgour JM, Li S, Sarin KY. Hidradenitis suppurativa in patients of color is associated with increased disease severity and healthcare utilization: a retrospective analysis of 2 US cohorts. JAAD Int. 2021;3:42-52.
4. Lee DE, Clark AK, Shi VY. Hidradenitis suppurativa: disease burden and atiology in skin of color. Dermatology. 2018;233(6):456-461.
5. Taylor SC, Elbuluk NM. Taylor and Elbuluk’s Color Atlas and Synopsis for Skin of Color. McGraw Hill; 2023;23:167.
*Photo credit: SCIENCE PHOTO LIBRARY.
06:03-06:09
Music
06:09-06:13
Music
Cultural Humility
Discover how approaching patient care through the perspective of cultural humility can make a difference in addressing unmet needs to achieve greater healthcare access.
Dr. ACKERMAN:
Hey!
Dr. DESAI:
So good to see you. I'm looking forward to this dialogue.
Dr. ACKERMAN:
So am I.
Dr. DESAI:
This will be great.
Dr. DESAI:
Cultural humility is so critical to our practices. It's not only important for ourselves as the ones providing care, but most importantly, to ensure that we have the highest-quality relationship and ultimate patient outcomes between our patients. And for me, I sort of think about cultural humility in the lens of compassion, caring, and really being able to ask the right questions so that you can continue to think about how does that skin disease relate to this patient's background, how does this patient's background relate to how they're going to be able to provide care for themselves once they leave this office visit?
Dr. ACKERMAN:
Yeah, I couldn't agree with you more. Cultural competency takes the cultural humility piece, which is what demands an interest and appreciation for understanding patients' preferences and biases and choices and actually implementing that into the patient care delivery process. So, it requires a lot of listening and then that translation of, "how can I execute?" That's the competence part—what this patient really needs and what their demands may be based on their cultural background and preferences.
Dr. DESAI:
I love that because you're right. They're so intertwined and yet also unique and different. And to your point, I think cultural competency, what I often think about it is when you're actually present, when you're there using that background of compassion and care, ultimately becoming more humble and having that humility.
Dr. ACKERMAN:
100%. We're all so visual. We're dermatologists. We're in the room and we're making assessments just with our eyes without even having a conversation. But I always like to think that we become that much better as dermatologists when we use not just our eyes, but our ears. We actually ask openended questions. We listen to their answers that pertain specifically to them, and then it becomes this lifelong process for us of just getting better. With every story, we get to learn something else, something new that we wouldn't ever have imagined potentially possible. But we can then gain an appreciation and then turn it around into competency where we deliver care that's much more patient specific.
And what's been the best part of it all is, you know, we do this because we want to be better at giving patients what they need, but in turn, the satisfaction we get in the provision of care model just becomes that much more rich.
Dr. DESAI:
So, I think the cultural humility component of dealing with patients who have been marginalized or from diverse background or let's say, even more broadly, skin of color, why is it important to that individual encounter? And one of the things that I think about when I'm in these visits, which I'm sure you do as well, is how am I going to make sure that what I'm saying to that patient actually translates into that person advocating for themselves once they leave the clinic, leave the setting, go home and start using their medication.
Are they going to understand what their skin disease really is? Are they going to be able to be compliant? Are they going to follow up? I think what I've learned through a lot of this is that many of our patients with skin of color, in many of their experience in the healthcare community, oftentimes don't feel heard. They don't feel validated.
They don't really feel like the clinician truly understood what was going on with their hair condition, or with their skin condition, or even if they had a skin condition. If you don't understand what it is and don't think that the clinician understands you, what gives you faith to actually fulfill the treatment and remain compliant?
Dr. ACKERMAN:
I tend to look at sometimes these visits where you walk into a room and you recognize that there's just this gap. There might be fear, there might be anxiety, there could be distrust. And really, what I try to do from the very beginning is close this gap. I feel like I'm in, you know, the ten-by-ten room. I've got my ten minutes or whatever it might be with them. And the first thing I need to do is get close. I need to make sure that they understand I'm there. I'm with them on the journey. You know, sometimes it'shands on their knees. Sometimes I shake a hand, and I hold it for a little longer.
Dr. DESAI:
Yes.
Dr. ACKERMAN:
Something that just tries to close that delta and let them know I'm in this with them. And then I can ask the right questions, and they're willing to answer them. That that fear gap tends to melt away. And we have this enormous gift. We've got a skill set that's so broad and can be distributed so well if we are still willing, with every one of these patient visits, in a culture that may be different than our own, or in a skin tone that's different than our own, to grow a little, to understand what their journey has been thus far, why do they maybe feel like they've been passed along they've been given ten answers to the same problem? And so that we can get closer to them and embrace that trust opportunity.
Dr. DESAI:
And a lot of times I think this gets challenging when we're educating our colleagues, because a lot of what we're talking about implies that this takes an inordinate amount of time during that visit, but it doesn't have to take 20, 30, 40 minutes to do that. Simple things like you said, which I loved, that personal connection, that touch, asking the probing question, but asking it in a way that doesn't seem like you're investigating and being inquisitive, asking more because you actually want to know the answer.
Dr. ACKERMAN:
Yeah, and asking for feedback, you know, I will ask a patient at the end of, you know, maybe, maybe I've been in their business, and I've looked at them and I've, you know, I've had physical touch. I feel close enough. I can say, okay, so tell me, how do you feel about that whole treatment plan we just went through?
Give them that open-ended opportunity to answer and render an opinion. I find my job the best job in the world. And I honestly feel like it gets more fun over time as I continue to embrace the learning opportunity that I'm given in lots of ways, that still means understanding better how to be culturally humble and competent. My visits become more fulfilling and also more fun. I'm having, you know, relationships with patients that, you know, we're talking about things I wouldn't have necessarily known that we could talk about or that we would want to talk about, but we're doing that all in the scope of providing care. It's not taking any more time. We're having this conversation while we're doing the exam, while we're filling out paperwork. You know, it just has become a much more fulfilling experience. And I've grown a ton.
Dr. DESAI:
And I like how you said that a lot of this happens naturally in the interaction, just how we're interacting today.
Dr. ACKERMAN:
Sure.
Dr. DESAI:
And it's the same concept. You're not necessarily interacting with another colleague. You're interacting with the patient, but you're doing it in a way where the patient knows there's not a necessarily a hierarchy in the room, that this is a discussion amongst each other and a joint decision-making process.
I think that term joint decision-making is really apt for that. You know, in our practice, similar to I know what you do, Lindsay, we, we oftentimes try to take note. Does the patient have a religious holiday or a religious preference that something a certain time of year? We make notes of that, just as a sidebar in the chart. So when I go in, I know a little bit more about where that person is in their personal journey. And could that help me better understand where they are?
Another example: we have a lot of patients who come in with tattoos. In many cultures, tattoos aren't there for cosmetic. They're there for cultural, religious significance, and diving a little bit and asking those questions. Oh, that's an interesting mark. Tell me more about it. Is that something that you did out of interest or necessity? Those are just small things that we try to do to implement some of these practices into our patient charts, and more as a note to me.
Dr. ACKERMAN:
For some, I could imagine when they're hearing us talk about this, that it could sound almost daunting, like, oh, how do I pivot? I really want to just comment on that and say what I mean by my job has become more fun is that pivot piece becomessomething I'm excited about. Now, you know, I have those notes in my chart also, and it just makes me feel like I know them better and…
Dr. DESAI:
Right.
Dr. ACKERMAN:
…in a way that, you know, if I didn't ask those questions initially, I would never know that about them. And so, I feel almost empowered as, as a person that I have that knowledge, that I know them as a human a little bit, you know, more delicately, and more specifically
Dr. DESAI:
And guess what, that means we've both learned something as well. Right? I mean, we've learned from our patients. A lot of times, one of my mentors in med school always said, your patients will tell you everything you need to know if you just listen
Dr. ACKERMAN:
My mentor said exactly the same thing.
Dr. DESAI:
So true.
Dr. ACKERMAN:
She said, you better listen to your patients. They will tell you everything you need to know.
Dr. DESAI:
Yeah, I love that.
Dr. ACKERMAN:
Yeah.
Advancing Care with Cultural Humility: What is Cultural Humility?
Dr. Ackerman and Dr. Desai discuss the concept of cultural humility, how it changes clinical perspective, and how it impacts the patient experience.
Dr. ACKERMAN:
Hey!
Dr. DESAI:
So good to see you. I'm looking forward to this dialogue.
Dr. ACKERMAN:
So am I.
Dr. DESAI:
This will be great.
Dr. DESAI:
Cultural humility is so critical to our practices. It's not only important for ourselves as the ones providing care, but most importantly, to ensure that we have the highest-quality relationship and ultimate patient outcomes between our patients. And for me, I sort of think about cultural humility in the lens of compassion, caring, and really being able to ask the right questions so that you can continue to think about how does that skin disease relate to this patient's background, how does this patient's background relate to how they're going to be able to provide care for themselves once they leave this office visit?
Dr. ACKERMAN:
Yeah, I couldn't agree with you more. Cultural competency takes the cultural humility piece, which is what demands an interest and appreciation for understanding patients' preferences and biases and choices and actually implementing that into the patient care delivery process. So, it requires a lot of listening and then that translation of, "how can I execute?" That's the competence part—what this patient really needs and what their demands may be based on their cultural background and preferences.
Dr. DESAI:
I love that because you're right. They're so intertwined and yet also unique and different. And to your point, I think cultural competency, what I often think about it is when you're actually present, when you're there using that background of compassion and care, ultimately becoming more humble and having that humility.
Dr. ACKERMAN:
100%. We're all so visual. We're dermatologists. We're in the room and we're making assessments just with our eyes without even having a conversation. But I always like to think that we become that much better as dermatologists when we use not just our eyes, but our ears. We actually ask openended questions. We listen to their answers that pertain specifically to them, and then it becomes this lifelong process for us of just getting better. With every story, we get to learn something else, something new that we wouldn't ever have imagined potentially possible. But we can then gain an appreciation and then turn it around into competency where we deliver care that's much more patient specific.
And what's been the best part of it all is, you know, we do this because we want to be better at giving patients what they need, but in turn, the satisfaction we get in the provision of care model just becomes that much more rich.
Dr. DESAI:
So, I think the cultural humility component of dealing with patients who have been marginalized or from diverse background or let's say, even more broadly, skin of color, why is it important to that individual encounter? And one of the things that I think about when I'm in these visits, which I'm sure you do as well, is how am I going to make sure that what I'm saying to that patient actually translates into that person advocating for themselves once they leave the clinic, leave the setting, go home and start using their medication.
Are they going to understand what their skin disease really is? Are they going to be able to be compliant? Are they going to follow up? I think what I've learned through a lot of this is that many of our patients with skin of color, in many of their experience in the healthcare community, oftentimes don't feel heard. They don't feel validated.
They don't really feel like the clinician truly understood what was going on with their hair condition, or with their skin condition, or even if they had a skin condition. If you don't understand what it is and don't think that the clinician understands you, what gives you faith to actually fulfill the treatment and remain compliant?
Dr. ACKERMAN:
I tend to look at sometimes these visits where you walk into a room and you recognize that there's just this gap. There might be fear, there might be anxiety, there could be distrust. And really, what I try to do from the very beginning is close this gap. I feel like I'm in, you know, the ten-by-ten room. I've got my ten minutes or whatever it might be with them. And the first thing I need to do is get close. I need to make sure that they understand I'm there. I'm with them on the journey. You know, sometimes it'shands on their knees. Sometimes I shake a hand, and I hold it for a little longer.
Dr. DESAI:
Yes.
Dr. ACKERMAN:
Something that just tries to close that delta and let them know I'm in this with them. And then I can ask the right questions, and they're willing to answer them. That that fear gap tends to melt away. And we have this enormous gift. We've got a skill set that's so broad and can be distributed so well if we are still willing, with every one of these patient visits, in a culture that may be different than our own, or in a skin tone that's different than our own, to grow a little, to understand what their journey has been thus far, why do they maybe feel like they've been passed along they've been given ten answers to the same problem? And so that we can get closer to them and embrace that trust opportunity.
Dr. DESAI:
And a lot of times I think this gets challenging when we're educating our colleagues, because a lot of what we're talking about implies that this takes an inordinate amount of time during that visit, but it doesn't have to take 20, 30, 40 minutes to do that. Simple things like you said, which I loved, that personal connection, that touch, asking the probing question, but asking it in a way that doesn't seem like you're investigating and being inquisitive, asking more because you actually want to know the answer.
Dr. ACKERMAN:
Yeah, and asking for feedback, you know, I will ask a patient at the end of, you know, maybe, maybe I've been in their business, and I've looked at them and I've, you know, I've had physical touch. I feel close enough. I can say, okay, so tell me, how do you feel about that whole treatment plan we just went through?
Give them that open-ended opportunity to answer and render an opinion. I find my job the best job in the world. And I honestly feel like it gets more fun over time as I continue to embrace the learning opportunity that I'm given in lots of ways, that still means understanding better how to be culturally humble and competent. My visits become more fulfilling and also more fun. I'm having, you know, relationships with patients that, you know, we're talking about things I wouldn't have necessarily known that we could talk about or that we would want to talk about, but we're doing that all in the scope of providing care. It's not taking any more time. We're having this conversation while we're doing the exam, while we're filling out paperwork. You know, it just has become a much more fulfilling experience. And I've grown a ton.
Dr. DESAI:
And I like how you said that a lot of this happens naturally in the interaction, just how we're interacting today.
Dr. ACKERMAN:
Sure.
Dr. DESAI:
And it's the same concept. You're not necessarily interacting with another colleague. You're interacting with the patient, but you're doing it in a way where the patient knows there's not a necessarily a hierarchy in the room, that this is a discussion amongst each other and a joint decision-making process.
I think that term joint decision-making is really apt for that. You know, in our practice, similar to I know what you do, Lindsay, we, we oftentimes try to take note. Does the patient have a religious holiday or a religious preference that something a certain time of year? We make notes of that, just as a sidebar in the chart. So when I go in, I know a little bit more about where that person is in their personal journey. And could that help me better understand where they are?
Another example: we have a lot of patients who come in with tattoos. In many cultures, tattoos aren't there for cosmetic. They're there for cultural, religious significance, and diving a little bit and asking those questions. Oh, that's an interesting mark. Tell me more about it. Is that something that you did out of interest or necessity? Those are just small things that we try to do to implement some of these practices into our patient charts, and more as a note to me.
Dr. ACKERMAN:
For some, I could imagine when they're hearing us talk about this, that it could sound almost daunting, like, oh, how do I pivot? I really want to just comment on that and say what I mean by my job has become more fun is that pivot piece becomessomething I'm excited about. Now, you know, I have those notes in my chart also, and it just makes me feel like I know them better and…
Dr. DESAI:
Right.
Dr. ACKERMAN:
…in a way that, you know, if I didn't ask those questions initially, I would never know that about them. And so, I feel almost empowered as, as a person that I have that knowledge, that I know them as a human a little bit, you know, more delicately, and more specifically
Dr. DESAI:
And guess what, that means we've both learned something as well. Right? I mean, we've learned from our patients. A lot of times, one of my mentors in med school always said, your patients will tell you everything you need to know if you just listen
Dr. ACKERMAN:
My mentor said exactly the same thing.
Dr. DESAI:
So true.
Dr. ACKERMAN:
She said, you better listen to your patients. They will tell you everything you need to know.
Dr. DESAI:
Yeah, I love that.
Dr. ACKERMAN:
Yeah.
Dr. ACKERMAN:
You know this shared decision-making that we, that we are fostering in our patient visits by being both culturally humble and competent, allows the patient to embrace this process from an empowered perspective.
Dr. DESAI:
I really like that you used the word empowered because I feel that if the patient feels empowered, that they were part of the decision. Guess what? They're more likely to actually follow through on the treatment. Come back and see you, stay consistent, and really stay focused on the fact that these, many of these things that they're being treated for are chronic and require long term, which means compliance is key, but you can't get there unless you really have that built-in connection and trust.
Dr. DESAI:
We also, I think, incorporate a lot of that into wanting to make sure specific skin diseases are addressed more uniquely. I mean, we as dermatologists, we treat, what, 3000-plus skin diseases of skin, hair, and nails. There can't be a one-size-fits-all approach to all 3000. So how do you make that more customizable and more unique?
Dr. DESAI:
I'll just give you one tangible example of some of our vitiligo patients, for example, that come from a Middle Eastern background. Many of my female patients from that part of the world that I see oftentimes don't want me necessarily examining every part of their body. There's a comfort level with the male physician. Even if we had a female chaperone in the room, a lot of times in those scenarios, we ask for photographs, are we allowed to have another person step in, take pictures of your lesions? Can I then look at it, and can we talk about it a little bit further? That then brings those barriers down and allows for us to get a little bit deeper.
Dr. ACKERMAN:
That's a perfect example. That sensitivity in recognizing where there's a gap in what otherwise is just our general workflow, you know, and how you can accommodate it without it being a burden on you or your staff or the office flow. It can be simple. It just has to be thoughtful. It just has to be something that we attend to.
Dr. ACKERMAN:
I mean, I'm vulnerable in front of patients. Sometimes I have to tell them, I'm not sure what this might be. I'm not sure what the next step is going to be. I'm not going to give up. And I want to, you know, potentially consider that we do this next, or we try this. But, I have found over time, this piece of being vulnerable with someone, being willing to learn about them primarily, it opens up that ability to be vulnerable and just be truthful and a holistically comprehensive and conscientious physician on all fronts.
Dr. DESAI:
And asking those questions. Right? Can I check this part of your body? Am I allowed to take pictures? Is there something that you need to tell me that would make you feel more comfortable? Is there something private that I haven't asked you yet? I think sharing a lot of that has definitely helped lower barriers.
Sometimes you don't get there, and I think that's okay as well, because now you know the patient's limitations and then you can sort of temper your behaviors around that. I expect myself to continue to get better and better as I learn more and more. And a lot of times what I learn from one patient is ultimately what I translate to the next patient
Dr. ACKERMAN:
You know, I even embarked on taking a self-awareness biases online questionnaire because I was just curious, you know, having invested a lot of my professional life impassioned to try to bring in those that otherwise are left out. I wanted to see how good am I or not good at, am I at having my own sort of unperceived but present biases. So, I've pursued that. I've also really tried to engage in making sure that I have adequate text references or visual references of some sort…
Dr. DESAI:
Sure.
Dr. ACKERMAN:
…to stay up to par on really seeing skin of color a lot, so that I'm not necessarily just relying on someone with skin of color walking in the door and giving me that experience.
Dr. DESAI:
I really like that you kind of did that self-awareness kind of exercise. I've done those as well. They're super helpful, sometimes brutally honest.
Dr. ACKERMAN:
Humbling, for sure.
Dr. DESAI:
Speaking of humility, right.
Dr. ACKERMAN:
Yeah.
Dr. DESAI:
One of the things for me that's been really interesting is getting involved in knowing I wanted the skin of color emphasis in my practice, getting involved with organizations in dermatology, the AAD, the Skin of Color Society, the NMA, all of these other groups that really help to elevate research and mentorship, I think, is the most important thing, is getting involved with other dermatology mentors who have kind of groomed and guided me. And now paying that forward with residents and medical students I work with.
Dr. ACKERMAN:
Now, there are so many that are out there that really are wide open for broad participation on a number of fronts. Whether you want to be someone who mentors or you actually want to be a mentee. There are opportunities in all of these organizations to do that.
Dr. DESAI:
And I think the other piece that we kind of touched on was doing it in our day-to-day practices, making sure we have culturally competent staff, recruiting staff who maybe have their own lived experiences and diverse backgrounds. Documenting your charts accordingly, giving yourself reminders. All of those things I think are really, really important.
Dr. ACKERMAN:
And frankly, even just doing this, this module.
Dr. DESAI:
This is all part of it.
Dr. ACKERMAN:
Exactly.
Dr. DESAI:
Yeah. I think the important messages here are building trust, creating rapport, creating a comfort level where the patient feels comfortable asking you questions, and you feel comfortable asking questions that may be probing, but not there to impart any sort of harshness or critique.
Dr. ACKERMAN:
Or judgement.
Dr. DESAI:
Judgment is so real for many of these patients, because they have a lot of distrust in the healthcare ecosystem from their past experiences. My job is to try to break that down, and if I can do that, that patient experience is just so much more better.
Dr. ACKERMAN:
And from the very get-go, we can do that in such simple ways by, you know, again, getting close to someone, decreasing the power differential by letting them sit a little bit more elevated than you, holding their hand for an extra second while you're talking. It takes no extra time, but it lets them know that you're there. The eye contact I find incredibly important.
Dr. DESAI:
One of the things that we always want to keep in mind when practicing cultural humility and competency is the patient's own individual experience with how they want to be treated in terms of the actual treatment plan, let's say. So, we talked earlier about stigmatizing skin diseases, but it could be as something on the spectrum of acne and scarring or vitiligo in a certain anatomic site.
Dr. DESAI:
You know, asking patients, is there a part of your skin disease that bugs you the most? Is there a part of the body that you're most concerned about wanting to improve? Or would you rather me try to fix everything? I oftentimes say, do you want me to fix it all? Or is there an area that bugs you more? And then I tell them, this is what I want to do. Is that aligned with what you want me to do? And asking those questions I think is really important.
Dr. ACKERMAN:
And sometimes when I recognize, again, through this whole humility process, that maybe I don't even know the right questions to ask, I like to open it up with a very open-ended question of just how does all of this sound to you? You know, how does this treatment plan seem to you? Is this going to work with your life?
Dr. DESAI:
Take the opportunity to learn about cultural practices. I know we've talked about hair care practices. What about practices like, do you use certain body products? Are there herbals? Are there cultural products involved? What kind of moisturizers? Do you use special botanical oils? In many cultures, for example, in the Indian culture, many patients use mustard seed oil and henna products, which is very culturally appropriate.
But those products may have reactions to what you're trying to prescribe and may not be the right choice. So, I think the list goes on in terms of really probing and really getting in there and getting that information.
Advancing Care with Cultural Humility: Embracing Cultural Humility
Dr. Desai and Dr. Ackerman talk about how working from a perspective of cultural humility changes their behaviors, empowers patients, and enriches their own clinical experience.
Dr. ACKERMAN:
You know this shared decision-making that we, that we are fostering in our patient visits by being both culturally humble and competent, allows the patient to embrace this process from an empowered perspective.
Dr. DESAI:
I really like that you used the word empowered because I feel that if the patient feels empowered, that they were part of the decision. Guess what? They're more likely to actually follow through on the treatment. Come back and see you, stay consistent, and really stay focused on the fact that these, many of these things that they're being treated for are chronic and require long term, which means compliance is key, but you can't get there unless you really have that built-in connection and trust.
Dr. DESAI:
We also, I think, incorporate a lot of that into wanting to make sure specific skin diseases are addressed more uniquely. I mean, we as dermatologists, we treat, what, 3000-plus skin diseases of skin, hair, and nails. There can't be a one-size-fits-all approach to all 3000. So how do you make that more customizable and more unique?
Dr. DESAI:
I'll just give you one tangible example of some of our vitiligo patients, for example, that come from a Middle Eastern background. Many of my female patients from that part of the world that I see oftentimes don't want me necessarily examining every part of their body. There's a comfort level with the male physician. Even if we had a female chaperone in the room, a lot of times in those scenarios, we ask for photographs, are we allowed to have another person step in, take pictures of your lesions? Can I then look at it, and can we talk about it a little bit further? That then brings those barriers down and allows for us to get a little bit deeper.
Dr. ACKERMAN:
That's a perfect example. That sensitivity in recognizing where there's a gap in what otherwise is just our general workflow, you know, and how you can accommodate it without it being a burden on you or your staff or the office flow. It can be simple. It just has to be thoughtful. It just has to be something that we attend to.
Dr. ACKERMAN:
I mean, I'm vulnerable in front of patients. Sometimes I have to tell them, I'm not sure what this might be. I'm not sure what the next step is going to be. I'm not going to give up. And I want to, you know, potentially consider that we do this next, or we try this. But, I have found over time, this piece of being vulnerable with someone, being willing to learn about them primarily, it opens up that ability to be vulnerable and just be truthful and a holistically comprehensive and conscientious physician on all fronts.
Dr. DESAI:
And asking those questions. Right? Can I check this part of your body? Am I allowed to take pictures? Is there something that you need to tell me that would make you feel more comfortable? Is there something private that I haven't asked you yet? I think sharing a lot of that has definitely helped lower barriers.
Sometimes you don't get there, and I think that's okay as well, because now you know the patient's limitations and then you can sort of temper your behaviors around that. I expect myself to continue to get better and better as I learn more and more. And a lot of times what I learn from one patient is ultimately what I translate to the next patient
Dr. ACKERMAN:
You know, I even embarked on taking a self-awareness biases online questionnaire because I was just curious, you know, having invested a lot of my professional life impassioned to try to bring in those that otherwise are left out. I wanted to see how good am I or not good at, am I at having my own sort of unperceived but present biases. So, I've pursued that. I've also really tried to engage in making sure that I have adequate text references or visual references of some sort…
Dr. DESAI:
Sure.
Dr. ACKERMAN:
…to stay up to par on really seeing skin of color a lot, so that I'm not necessarily just relying on someone with skin of color walking in the door and giving me that experience.
Dr. DESAI:
I really like that you kind of did that self-awareness kind of exercise. I've done those as well. They're super helpful, sometimes brutally honest.
Dr. ACKERMAN:
Humbling, for sure.
Dr. DESAI:
Speaking of humility, right.
Dr. ACKERMAN:
Yeah.
Dr. DESAI:
One of the things for me that's been really interesting is getting involved in knowing I wanted the skin of color emphasis in my practice, getting involved with organizations in dermatology, the AAD, the Skin of Color Society, the NMA, all of these other groups that really help to elevate research and mentorship, I think, is the most important thing, is getting involved with other dermatology mentors who have kind of groomed and guided me. And now paying that forward with residents and medical students I work with.
Dr. ACKERMAN:
Now, there are so many that are out there that really are wide open for broad participation on a number of fronts. Whether you want to be someone who mentors or you actually want to be a mentee. There are opportunities in all of these organizations to do that.
Dr. DESAI:
And I think the other piece that we kind of touched on was doing it in our day-to-day practices, making sure we have culturally competent staff, recruiting staff who maybe have their own lived experiences and diverse backgrounds. Documenting your charts accordingly, giving yourself reminders. All of those things I think are really, really important.
Dr. ACKERMAN:
And frankly, even just doing this, this module.
Dr. DESAI:
This is all part of it.
Dr. ACKERMAN:
Exactly.
Dr. DESAI:
Yeah. I think the important messages here are building trust, creating rapport, creating a comfort level where the patient feels comfortable asking you questions, and you feel comfortable asking questions that may be probing, but not there to impart any sort of harshness or critique.
Dr. ACKERMAN:
Or judgement.
Dr. DESAI:
Judgment is so real for many of these patients, because they have a lot of distrust in the healthcare ecosystem from their past experiences. My job is to try to break that down, and if I can do that, that patient experience is just so much more better.
Dr. ACKERMAN:
And from the very get-go, we can do that in such simple ways by, you know, again, getting close to someone, decreasing the power differential by letting them sit a little bit more elevated than you, holding their hand for an extra second while you're talking. It takes no extra time, but it lets them know that you're there. The eye contact I find incredibly important.
Dr. DESAI:
One of the things that we always want to keep in mind when practicing cultural humility and competency is the patient's own individual experience with how they want to be treated in terms of the actual treatment plan, let's say. So, we talked earlier about stigmatizing skin diseases, but it could be as something on the spectrum of acne and scarring or vitiligo in a certain anatomic site.
Dr. DESAI:
You know, asking patients, is there a part of your skin disease that bugs you the most? Is there a part of the body that you're most concerned about wanting to improve? Or would you rather me try to fix everything? I oftentimes say, do you want me to fix it all? Or is there an area that bugs you more? And then I tell them, this is what I want to do. Is that aligned with what you want me to do? And asking those questions I think is really important.
Dr. ACKERMAN:
And sometimes when I recognize, again, through this whole humility process, that maybe I don't even know the right questions to ask, I like to open it up with a very open-ended question of just how does all of this sound to you? You know, how does this treatment plan seem to you? Is this going to work with your life?
Dr. DESAI:
Take the opportunity to learn about cultural practices. I know we've talked about hair care practices. What about practices like, do you use certain body products? Are there herbals? Are there cultural products involved? What kind of moisturizers? Do you use special botanical oils? In many cultures, for example, in the Indian culture, many patients use mustard seed oil and henna products, which is very culturally appropriate.
But those products may have reactions to what you're trying to prescribe and may not be the right choice. So, I think the list goes on in terms of really probing and really getting in there and getting that information.
Dr. ACKERMAN:
You know, I think that the first and most important thing that one can embrace along this journey is just to recognize that there's room to grow. It's okay to not be perfect at this point in your career, and maybe the goal should never to be perfect. It's just always to be open to getting better.
Dr. DESAI:
So I'm going to actually start doing that now because I think that's important. And self-critique is important. I think just to take a step back, one of the things that your comment reminded me of is you have to want to care to improve, but we have to be also realistic that this is maybe a topic that not every clinician really feels is important, but how can we make it relevant to that clinician as well, that we all have to practice cultural humility and cultural competency?
Dr. DESAI:
And the adage I always say is at some point, each of us are going to be patients as well. We may have a culturally diverse physician or provider providing us care. You may be from that background; you may have a family member from that background. So, I think we're all affected by it. And we've got to invest in wanting to learn it.
Dr. ACKERMAN:
And you could easily look at all of this content and say, well, isn't this just attributable to any particular patient? We want to be sensitive to the patient. We want to be kind and caring, but more so when it comes to those who have been left out of the fold, or who may have a more difficult journey to getting to us, or that have been historically marginalized by virtue of stigma or access or resources giving them that embrace of our cultural humility and ultimately, our cultural competence, really creates an environment where patients can thrive, and we can thrive. This is like the beginning of the process, not the end.
Dr. DESAI:
You know, when we when we think about the teambased approach to care, that team is not just you and your nurse. That team is, goes way beyond. That includes your front office person, your checkout person, your billing person. A great example is insurance literacy and patients understanding how to navigate their benefits and how to navigate getting a medication, how to navigate what's a deductible, how to navigate, how to make an appointment for their family member.
Dr. DESAI:
All of those things, I don't have the time in my clinic to be able to do, but I've empowered my team, who I trust to do it and to do it in a really compassionate, caring way. And so I love what you said is that it's, it's follow the leader. But also sometimes for the patient, there's a comfort level with your office staff that's different from the comfort level with you as the physician.
Dr. ACKERMAN:
Right.
Dr. DESAI:
You know, there's that respect factor in many cultures. Their physicians are revered, where it's continued to be looked upon as leaders, and a lot of times that patient may be more comfortable talking in the hallway to my nurse or saying something to my checkout person. A lot of times I hear that later. Oh, by the way, this person said they really enjoyed this, or they didn't tell you this because of a certain reason.
Dr. ACKERMAN:
And especially when it comes to financial conversations. Not only am I poorly equipped to handle them, but there is a comfort zone that you can give. If your staff can be culturally sensitive, you can give that relationship to the patient and your staff member to have the conversation, which ultimately is much more fulfilling.
Dr. DESAI:
Yes.
Advancing Care with Cultural Humility: Fostering Patient-Centered Care
Dr. Ackerman and Dr. Desai discuss why cultural humility is a constant evolution—a process that involves looking inward in self-reflection and expanding outward to create a holistic patient-centered experience.
Dr. ACKERMAN:
You know, I think that the first and most important thing that one can embrace along this journey is just to recognize that there's room to grow. It's okay to not be perfect at this point in your career, and maybe the goal should never to be perfect. It's just always to be open to getting better.
Dr. DESAI:
So I'm going to actually start doing that now because I think that's important. And self-critique is important. I think just to take a step back, one of the things that your comment reminded me of is you have to want to care to improve, but we have to be also realistic that this is maybe a topic that not every clinician really feels is important, but how can we make it relevant to that clinician as well, that we all have to practice cultural humility and cultural competency?
Dr. DESAI:
And the adage I always say is at some point, each of us are going to be patients as well. We may have a culturally diverse physician or provider providing us care. You may be from that background; you may have a family member from that background. So, I think we're all affected by it. And we've got to invest in wanting to learn it.
Dr. ACKERMAN:
And you could easily look at all of this content and say, well, isn't this just attributable to any particular patient? We want to be sensitive to the patient. We want to be kind and caring, but more so when it comes to those who have been left out of the fold, or who may have a more difficult journey to getting to us, or that have been historically marginalized by virtue of stigma or access or resources giving them that embrace of our cultural humility and ultimately, our cultural competence, really creates an environment where patients can thrive, and we can thrive. This is like the beginning of the process, not the end.
Dr. DESAI:
You know, when we when we think about the teambased approach to care, that team is not just you and your nurse. That team is, goes way beyond. That includes your front office person, your checkout person, your billing person. A great example is insurance literacy and patients understanding how to navigate their benefits and how to navigate getting a medication, how to navigate what's a deductible, how to navigate, how to make an appointment for their family member.
Dr. DESAI:
All of those things, I don't have the time in my clinic to be able to do, but I've empowered my team, who I trust to do it and to do it in a really compassionate, caring way. And so I love what you said is that it's, it's follow the leader. But also sometimes for the patient, there's a comfort level with your office staff that's different from the comfort level with you as the physician.
Dr. ACKERMAN:
Right.
Dr. DESAI:
You know, there's that respect factor in many cultures. Their physicians are revered, where it's continued to be looked upon as leaders, and a lot of times that patient may be more comfortable talking in the hallway to my nurse or saying something to my checkout person. A lot of times I hear that later. Oh, by the way, this person said they really enjoyed this, or they didn't tell you this because of a certain reason.
Dr. ACKERMAN:
And especially when it comes to financial conversations. Not only am I poorly equipped to handle them, but there is a comfort zone that you can give. If your staff can be culturally sensitive, you can give that relationship to the patient and your staff member to have the conversation, which ultimately is much more fulfilling.
Dr. DESAI:
Yes.
Duration 3:19
What is Cultural Humility?
Dr. Barbosa and Dr. Ko introduce the concept of cultural humility, emphasizing the importance of understanding the patient’s perspective. They encourage HCPs to approach patients with an open mindset, express curiosity, and meet them where they are.
Duration 3:52
Walking Through the Patient Experience
Dr. Ko and Dr. Barbosa recommend an introspective approach for HCPs. They encourage HCPs to reflect on how patients perceive their surroundings in the doctor’s office, recognizing that the environment can significantly influence patient perceptions.
Duration 2:52
Communication: Being the Expert and the Curious
Dr. Ko and Dr. Barbosa delve into the interplay of confidence and curiosity during patient interactions, especially when seeking to understand cultural practices and beliefs.
Duration 2:24
Digging Deeper in Derm: An Example of Religious Beliefs
Dr. Ko provides valuable insights into the impact of religious practices on patient care decisions. He emphasizes that understanding and appreciating these practices can significantly enhance HCP interactions.
Duration 2:14
Patient Challenges: Learning From What You Don’t See
Dr. Barbosa discusses her encounters with patients who have hidden disabilities, which may not always be immediately apparent but can significantly impact the quality and outcome of the patient visit.
Understanding Cultural Humility in Healthcare
Discover practical ways you can put cultural humility into practice.

Stay Connected
to receive updates and new resources from Sides of My Skin.
References
- Girolomoni G, Busà VM. Flare management in atopic dermatitis: from definition to treatment. Ther Adv Chronic Dis. 2022;13:20406223211066728. Published 2022 Jan 13.
- Creadore, A., Desai, S., Li, S. J., Lee, K. J., Bui, A. N., Villa-Ruiz, C., Lo, K., Zhou, G., Joyce, C., Resneck, J. S., Jr, Seiger, K., & Mostaghimi, A. (2021). Insurance Acceptance, Appointment Wait Time, and Dermatologist Access Across Practice Types in the US. JAMA dermatology, 157(2), 181–188. https://doi.org/10.1001/jamadermatol.2020.5173
- Duniphin, D. (2023). Limited Access to Dermatology Specialty Care: Barriers and Teledermatology. Dermatology Practical & Conceptual, 13(1), e2023031. https://doi.org/10.5826/dpc.1301a31
- Shukla, M., Schilt-Solberg, M., & Gibson-Scipio, W. (2025). Medical Mistrust: A Concept Analysis. Nursing reports (Pavia, Italy), 15(3), 103. https://www.mdpi.com/2039-4403/15/3/103